Jaundice is an elevation of bilirubin levels in the blood which gives a yellow tinge to the baby’s skin.
Types of jaundice
-
Physiological
AKA Icterus neonatorum
Due to breakdown of excess red blood cells (RBC) and release of bilirubin.
-
Early Onset
ABO incompatibility
Due to maternal blood type O transfers to baby with blood type A or B.
-
Late Onset
AKA Breast milk jaundice
Due to the hormone in milk interferes with baby’s ability to eliminate bilirubin.
-
Pathological
Most commonly caused by:
– Liver disease or obstructed bile duct
– Infection
– Rh hemolytic disease
Physiological Vrs Pathological Jaundice

Physiological Jaundice
- Not visible in first 24 hours
- Rises slowly and peaks at day 3 or 4 of life
- Total bilirubin peaks at < 13 mg/dL
- Lab tests reveal predominance of unconjugated bilirubin
- Not visible after 10 days in the premature infant or 7 days in the full-term baby
Pathological Jaundice
- Visible during first 24 hours
- May rise quickly: > 5mg/dL/24 hours
- Total bilirubin > 13 mg/dL
- Greater amounts of conjugated bilirubin
- Visible jaundice persists after one week
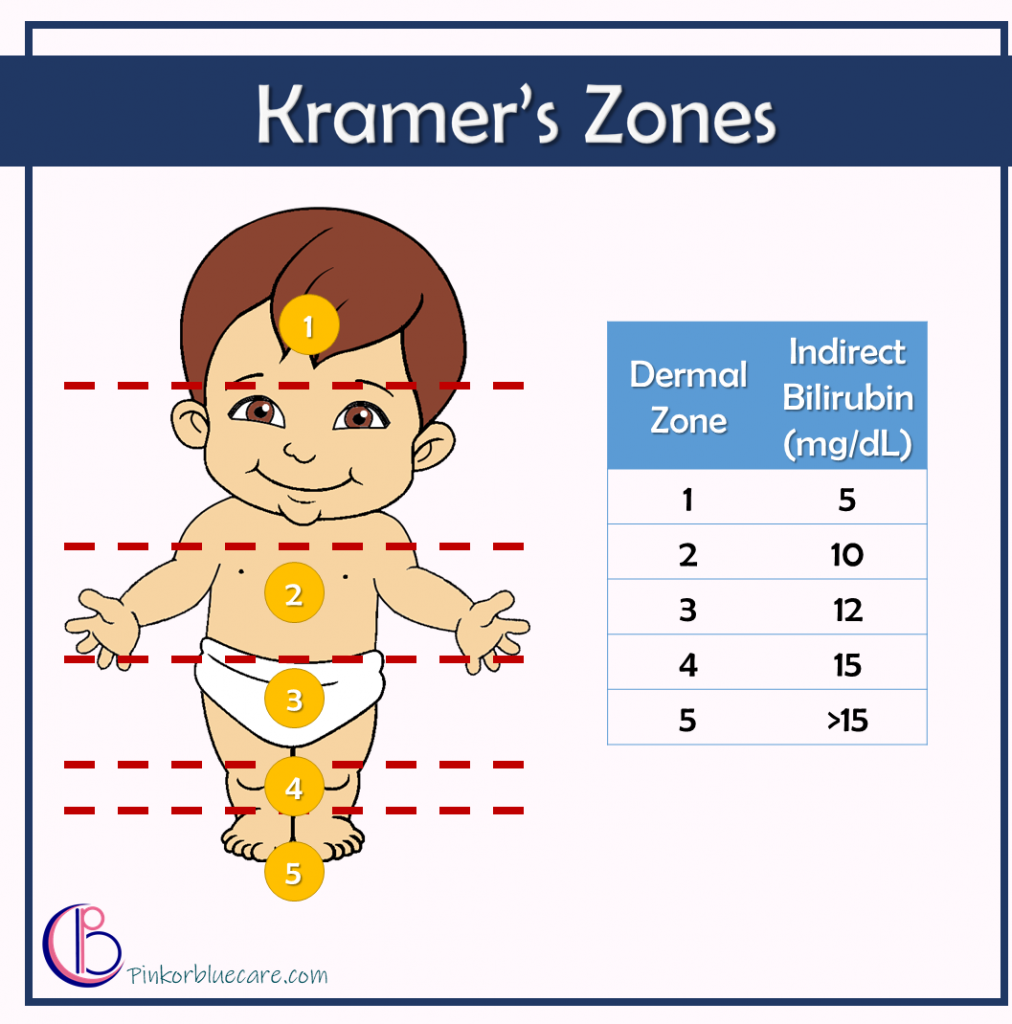
Jaundice Evaluation
Evaluate baby in a well-lighted room or close to a sunny window by gently pressing and blanching the skin to reveal the underlying color.
- The icterus will start on the head and face and move downward to the trunk and extremities, this is called cephalocaudal progression.
Kramer’s dermal icterus zones and serum indirect bilirubin level in a term infant is an useful tool to evaluate jaundice in a newborn.